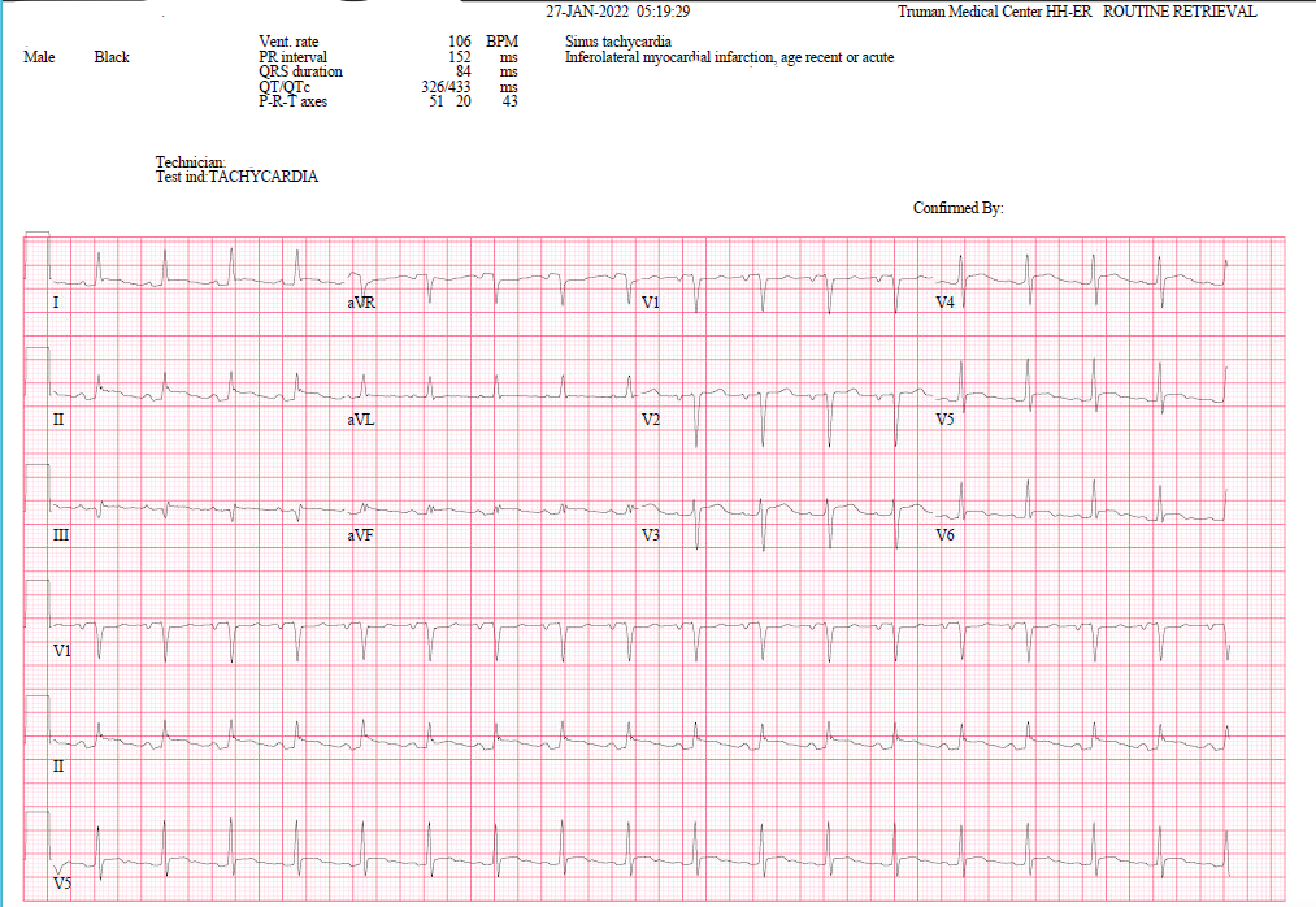
A 55-year-old man with worsening kidney functions presents with SOB. The ECG is most consistent with which diagnosis?
- Brugada syndrome.
- Acute Myocardial Infarction.
- Pericarditis.
- Normal variant early repolarization.
- Ventricular aneurysm.
- Hyperkalemia.
The right answer is:
3- Pericarditis
Explanation:
The ECG shows sinus rhythm and classic findings of acute pericarditis with diffuse (anterior-lateral and inferior distribution) ST-segment elevations (epicardial current of injury pattern) in leads I, II, III, aVF, and V3-V6. Lead aVR shows reciprocal ST depression (remember from quiz 1 that the isoelectric segment that you should compare to is the TP segment). Very subtle PR segment deviations that are discordant to the ST deviations (i.e., PR segment elevation in lead aVR and depression in the inferolateral leads) are due to a concomitant atrial injury current (refer to quiz 1 for a quick review on “current of injury”). The combination of findings strongly favors acute pericarditis, rather than the other choices given.
This patient, unfortunately, sustained a PEA cardiac arrest shortly and underwent emergency pericardiocentesis during resuscitation as he was having a tamponade. Fortunately, he survived the arrest and underwent a pericardial window procedure later.
The early repolarization pattern refers to normal variant ST elevations, most marked usually in leads V3-4 and not accompanied by PR segment shifts, as seen in the present case. In contrast, acute pericarditis’ ST elevations persist out to V5-V6 and limb leads. The presence of PR deviations (up in aVR and down in the inferolateral leads) with pericarditis is also often helpful.
Brugada’s syndrome consists of ST elevations in the right precordial leads (V1-V2 or V3) with a right bundle branch block appearing pattern. This pattern, which may be a marker of risk for ventricular tachyarrhythmias, is not present here.
Ventricular aneurysm after myocardial infarction may be associated with persistent ST-segment elevations usually with pathologic Q waves. The ST-segment elevations due to acute myocardial infarction or ventricular aneurysm are usually in one lead distribution (anterior/lateral vs. inferior/posterior). Reciprocal changes (i.e., slight ST depressions) may be present in the other lead set. In contrast, acute pericarditis usually doesn’t respect coronary artery distributions and usually extends to more than one territory (anterior-lateral-inferior) without Q waves or reciprocal changes (unless it’s post-infarction pericarditis with Q waves).
Take home message:
Pericarditis characteristic ECG changes:
- Widespread concave ST elevation (our patient didn't have the typical concave ST elevation) and PR depression throughout most of the limb leads (I, II, III, aVL, aVF) and precordial leads (V2-6) (Figure 1)
- ST depression and PR elevation in lead aVR (± V1) (Figure 2)
- Sinus tachycardia is also common in acute pericarditis due to pain and/or pericardial effusion.
NB. ST- and PR-segment changes are relative to the baseline formed by the T-P segment. The degree of ST elevation is typically modest (0.5 – 1mm).
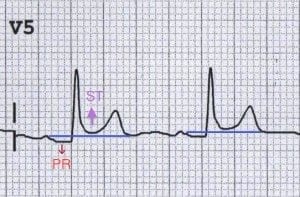
Figure 1: PR depression and ST elevation in V5
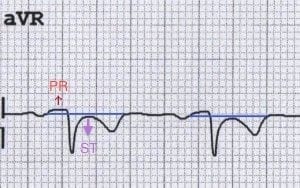
Figure 2: Reciprocal PR elevation and ST depression in aVR
Extra food for the brain
Stages of Pericarditis
Pericarditis is classically associated with ECG changes that evolve through four stages.
Stage 1 – widespread STE and PR depression with reciprocal changes in aVR (occurs during the first two weeks)
Stage 2 – normalization of ST changes; generalized T wave flattening (1 to 3 weeks)
Stage 3 – flattened T waves become inverted (3 to several weeks)
Stage 4 – ECG returns to normal (several weeks onwards)
NB. Less than 50% of patients progress through all four classical stages and the evolution of changes may not follow this typical pattern.
References:
- Nathanson LA, McClennen S, Safran C, Goldberger AL. ECG Wave-Maven: Self-Assessment Program for Students and Clinicians. http://ecg.bidmc.harvard.edu.
- Goldberger, Ary L., Zachary D. Goldberger, and Alexei Shvilkin. Clinical electrocardiography: a simplified approach e-book. Elsevier Health Sciences, 2017.
- Ed Burns and Robert Buttner. Life in the fast lane. https://litfl.com/pericarditis-ecg-library/